Not everyone is pleased with this blog. A couple of women, one of whom counsels breast cancer patients, have expressed outrage, which you will see as you read through these entries. But most of the commentss I have received are supportive, and I am grateful for those women who have taken the time to write to me. At least three of them decided to go elsewhere for their cancer care, and one actually canceled her pending appointment!
This blog exists to encourage you to choose your care wisely and avoid any doctor — like this one — who can’t or won’t provide quality care. The clues will be there at your first visit — if s/he is inconsiderate or brusque, brushes off your questions with vague or no answers, asks you what you did to get this cancer (he actually asked me that!), and/or hurries you out of the office, chances are the care they provide will be inadequate or even dangerous. We know that breast cancer can kill. . .but so can incompetent doctors — I learned that the hard way.

I was diagnosed with breast cancer on January 25, 2021. “Breast cancer” — those words paralyzed me with fear.
But only for a little while.
Once I realized that I wasn’t ready to die, I was ready to fight. Fortunately, I found immediate help at the Elizabeth Wende Breast Center in Henrietta, NY. This facility employs competent and compassionate caregivers and support staff. They did my entire workup — diagnostic mammogram, ultrasound, MRI, and biopsy — all in the same day, something the local hospitals take weeks to accomplish.
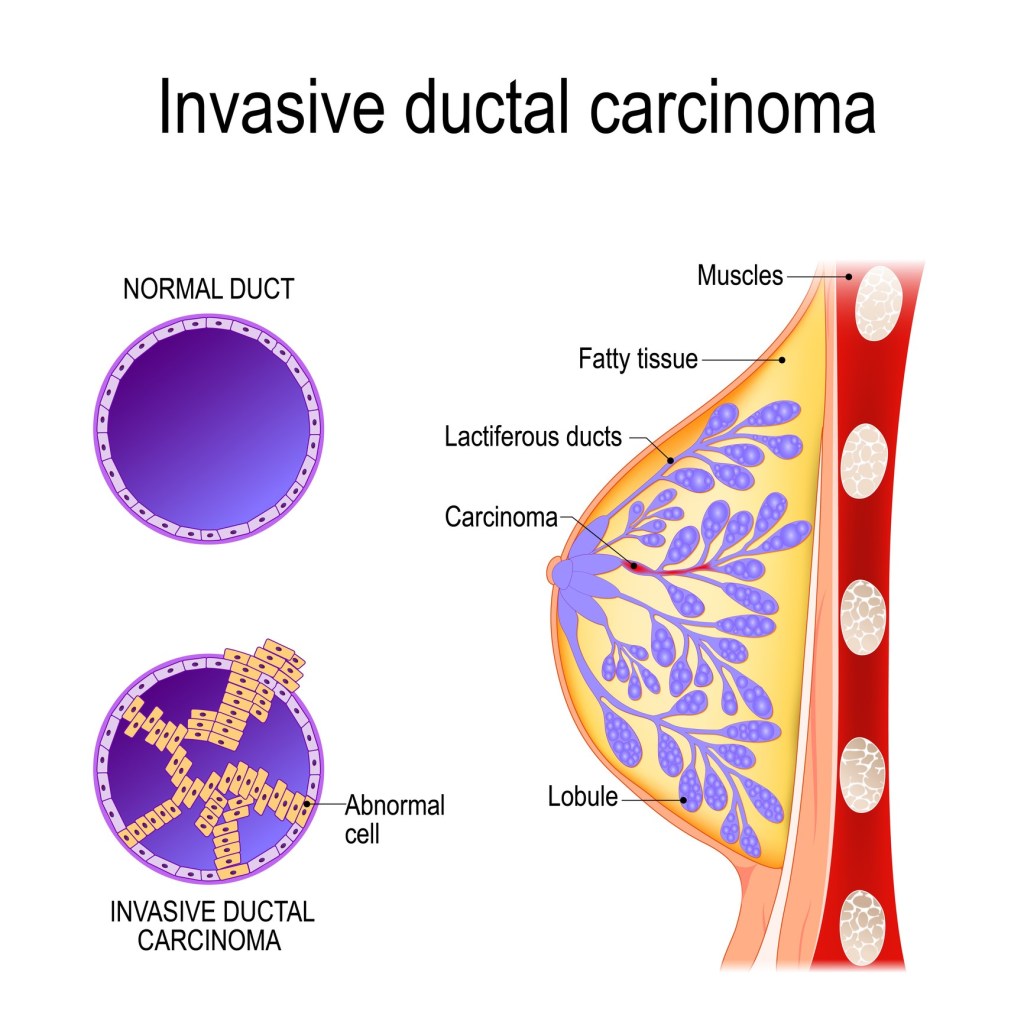
It was cancer, no doubt about it. EWBC sent me to an excellent surgeon at the Pluta Cancer Center run by the University of Rochester (NY), Jessica Gooch, MD, who performed a partial mastectomy and sentinal node biopsy. These revealed a node-negative stage I intraductal carcinoma with medullary features. She then referred me to a medical oncologist, Ajay Dhakal, MBBS.

(From https://www.urmc.rochester.edu/people/112361746-ajay-dhakal, August 2022)
Based on oncogene testing, Dr. Dhakal advised a short course of taxane chemotherapy, which he indicated would give me an excellent chance of living a long, disease-free life.
It would have, had he known what he was doing.
But he didn’t.
However, I didn’t know that. I trusted him. I bought some hats, shaved my head, and arrived tearfully but promptly for my first chemo treatment on March 11, 2021.

The chemo went well. I rested at home and waited for the legendary nausea and vomiting to begin, but it didn’t. Aside from some mild fatigue, I felt fine.
That is, until a few days later when I developed the sudden onset of severe abdominal pain and a fever of 103. I couldn’t eat anything without having an urgent liquid bowel movement only moments later.
Something was terribly wrong.
I called Dr. Dhakal, but he was unfazed. “This is only day 8,” he said. “Wait 4 days. By day 12 you will feel much better.”
However, I didn’t feel much better. The liquid bowel movements no longer occurred because any fecal matter produced by my bowel returned as vomitus. I got conflicting advice from the nurses at the infusion center, who all agreed nonetheless that I should “hang in there,” which I did until the prescribed 4-day wait ended on March 21. Two phone calls to Dr. Dhakal went unanswered, so I asked my neighbor to take me to the emergency room.
She took one look at me and called the ambulance.

I have only a few brief, disconnected memories of what happened next. I remember screaming in pain. I remember some foreign-looking doctor talking at me but I don’t remember what he said. I remember bandages piled so high on my abdomen that I could not see over them. I remember someone telling a group of others that “she’s assisting the respirator but let’s keep her on it for one more day.” I remember excruciating pain whenever the nurses came in to turn me; I was too weak to turn myself. I remember a tear rolling down my face but couldn’t lift my hand to wipe it away.
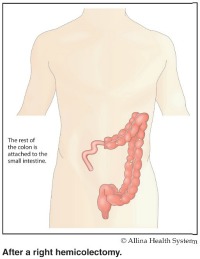
Thus began my recovery from typhlitis (neutropenic enterocolitis). This uncommon, life-threatening illness is a known complication of taxane chemotherapy, specifically docetaxel. If allowed to progress (as mine was, thank you Dr. Dhakal) typhlitis will attack the ileocecal junction (where the small intestine joins the large bowel), causing a hole (perforation) that spills dangerous toxins into the abdomen. Survival rates are in the 50-50 range, worse if the disease progresses to perforation.

Which mine did over those 4 fateful days. Thank you, Dr. Dhakal. You’ve been such a help.
The typhlitis destroyed the ileocecal junction and a good portion of my large and small intestine, causing massive infection, respiratory failure, and acute kidney injury. I required 2 life-saving surgeries, several rounds of potent antibiotics, and a ventilator to breathe for me when I was too sick to breathe on my own.
Again, I was one of the lucky ones. I survived. Most people with perforation don’t.
Recovery was slow. The trauma surgeon, Michael Vella, MD, was phenomenal. He saved my life by resecting the necrotic bowel and placing an end ileostomy.
Now, lots of people live with ostomies, sometimes for the rest of their lives, but I couldn’t bear to touch mine. I couldn’t even look at it without gagging. It took weeks of expert medical care from dedicated, patient, and well-trained others along with an additional hospitalization before I could penetrate that psychological barrier created when Dr. Dhakal refused to see me and instead advised that I “wait 4 days.”

Eventually, though, I did learn how to maintain and care for the ostomy. I even ordered the supplies myself, at the bargain price of about $300 per month.
Thank you, Dr. Dhakal, for this unique shopping experience. It’s money I likely would have wasted otherwise. . .you know, on things like utility bills. Or food.
Eight months later in November 2021, I was healed enough to undergo ostomy takedown, performed by the very skilled and very trusted Dr. Vella. For me, it was a difficult but much welcomed surgery. I looked forward to moving on and forgetting Dr. Dhakal and his sorry, sordid incompetence.
But wait, there’s more!

The 3 surgeries had each required an open approach. These being done in a relatively short period of time resulted in loss of abdominal domain with the development of multiple large herniations. I needed a fourth surgery to reduce the hernias and lyse the adhesions, which Dr. Vella carefully and skillfully performed on July 20, 2022. He then turned the surgery over to his colleague, Derek Bell, MD, who created bilateral rectus abdominus flaps to hold my abdominal contents in place. These two surgeons accomplished an excellent repair during a tedious 3-hour surgery.
Thank you, Dr. Dhakal, for not caring whether my guts fall out. And thank you, Dr. Vella and Dr. Bell, for making sure they don’t.
I am currently recovering from this last surgery. The staple line, like the others, extends from just below the tip of the xiphoid down to the symphysis pubis. It’s scabby and ugly but still healing. One of the JP drains was removed at my last followup visit, but the other continues to collect excessive fluid produced by the injured tissues. As of August 4, almost 3 weeks post surgery, I still empty about 25 ml of it several times a day and at least once in the middle of the night.
Thank you again, Dr. Dhakal. Your ignorance and incompetence has provided a novel opportunity for such extensive scarring that I can never wear a bathing suit lest I frighten little children (and probably some adults as well).
Given the results of all this Dhakal-inspired care, I am missing about a third of my lower GI tract. Whenever I eat, I have discomfort in my mid abdomen, so I consume smaller, more frequent meals in attempts to lessen it. My diet is limited to foods that will not stress my shortened bowel. I drink water almost constantly to replace that lost by inadequate bowel function. . .but not too much lest it interfere with electrolyte absorption.
I can’t wait to return to “normal,” whatever (and whenever) that might be.
Once again, thank you Dr. Dhakal. For everything. But can you quit helping me now? PLEASE?????
ALL of these surgeries, ALL of this angst, and ALL of this pain could have been avoided had Dr. Dhakal listened to me rather than dismiss me as some sort of chemo newbie who couldn’t take the side effects. No one expects him to predict who will or will not get typhlitis, but as a licensed, board-certified medical oncologist, he should have known how to diagnose it. He should have known that its symptoms differ markedly from those produced by chemotherapy, both in onset and character. At the very least he should have known that post-chemo fever demands prompt investigation. But he didn’t know any of this — or if he did, he didn’t care. Thankfully, the ER residents did — because THEY are the ones who diagnosed me. THEY knew that typhlitic symptoms and fecal vomitus are ALWAYS medical emergencies that simply cannot “wait 4 days” — and they acted accordingly, which is why I remain on this side of the grass.
But not Ajay Dhakal. No ma’am. He must’ve been absent the day they taught all that in medical school.
In fact, I learned (much later (in February of 2024) that an MBBS is an undergraduate degree available to anyone with some money and a grade average of C- (73.01). THAT is how “Dr.” Dhakal (barely) graduated from the Kathmandu College and Teaching Hospital — and he was stupid enough to brag about it on his LinkedIn page! (If only I had only known this before I trusted him!) So, I suppose it doesn’t matter if he missed a day or two of the undergraduate training, if the best he could do in a second-rate, 4-year school is C-. I am lucky to be living proof of his ignorance — I am sure, with such a stellar C- academic record and abysmal patient care practices, he will never be able to render anything resembling quality care.

But I digress.
So thank you, Dr. Dhakal, for creating, ignoring, and then donating my near-death experience to several alert ER residents who put their excellent training and education to work and thus saved my life.
Obviously, Dr. Dhakal doesn’t care about any of this. His arrogance protects his ignorance and excuses him from any and all consequences of it. Clearly he failed to perform his medical duties, but I suspect that, even if he was clever enough to distinguish a typhlitic patient from a hill of beans, he wouldn’t do a thing about it anyway, other than tempt fate by prescribing a dangerous 4-day wait.
Oh, did I say “arrogance?” Yes, I did. . .because this is the response I got when informing him of my diagnosis: “This has never happened to me before.”

Well, I beg to differ. This did not happen to YOU, you moron. It happened to ME. BECAUSE of you.
I did seek legal remedy but to no avail. You see, it is virtually impossible to for anyone in the profession to testify against a colleague. They don’t care about malpractice — all they care about is protecting each other — you know, “there but for the grace of God go I.” Unless, of course, they are swayed to the side of truth by a hefty chunk of change. . . which I don’t have and never will. The extensive critical care and surgeries I required have resulted in a large bill due and owing the UofR — I paid less than that for my house!
Thank you again, Dr. Dhakal! And thank you to the screwed-up legal system that protects you. And thanks, too, to the good ole USA, where ObamaCare does its best but cannot possibly keep up with the obscene profits that corporate medicine extorts from each and every patient unlucky enough to require its care.
Reporting him to UR Medicine Quality Control was equally futile. Their agent in the Patient Relations Department merely confirmed the symbiosis that exists between the institution and Dr. Dhakal. She easily absolved him of any and all negligence simply by blaming ME. It was my fault because I expected too much. It was my fault because I didn’t call him enough. It was my fault because I didn’t explain my symptoms enough. It was my fault because I wasn’t good enough — I don’t need validation, I need “psychiatric care.”
Thank you, Judy Barrett, BSN, for your shameful, victim-blaming diagnosis that relieves Ajay Dhakal of any responsibility arising from his callous, life-threatening incompetence — and ignores the long list of (over)charges that UR Medicine billed me for the privilege of saving me from same.
Is this why Ajay Dhakal remains on the UR Medicine staff? Because the poor-medical-care-requiring-more-medical-care he provides increases their bottom line?
Well, now, just wait a minute — maybe Judy’s right. Maybe I am crazy. But if so, who does she think made me this way?
What I would like to know is this: What was Ajay Dhakal doing when he advised me to “wait 4 days?” Was he having coffee with his wife or coworkers? Watching TV? Shopping at the mall or Trader Joe’s? Joking with friends? Playing golf? Making Facebook comments about Nepal’s tiger population? What makes any of these things more important than my life?
(I realize <<sigh>> that rhetorical questions like these might come across as somewhat sarcastic. . .)
I have every reason to believe that these and other triviata will remain more important than the lives of any of the breast cancer patients this man continues to see. This is the narcissistic power that results when ignorance is tinged with arrogance. This is why there is something called the Dunning-Kruger effect. This is why Ajay Dhakal gets away with near-murder — and maybe even murder.
I write this essay for one reason and one reason only: To do what Marcia Krebs, M.D., Chief of Medical Oncology at the Pluta Cancer Center, Jonathan Friedberg, M.D., M.M.Sc. at Wilmot Cancer Institute, and UR Medicine’s Patient Advocate Judy Barrett, B.S.N., all refuse to do, and that is to alert other women in the Rochester, NY area seeking breast cancer treatment to the dangers posed by Dr. Dhakal’s carelessness and incompetence, which the University of Rochester nonetheless promotes as its trademarked “Meliora” and “Medicine of the Highest Order.” In my experience, no woman can safely entrust him with their cancer care because he doesn’t see them as patients — they are his hapless victims and he the innocent (but narcissistic) Good Samaritan. He doesn’t cause them any problems; THEY are the ones who cause problems for HIM. That’s why things like typhlitis happen to him — and not his patients.

I am disgusted every time I see that ignorant smirk on his face (From https://issuu.com/urmc/docs/ctsi_3728_ur_ctsi_annual_report_2021_2022_issuu)
As long as UR Medicine and its associated cancer centers continue to employ dangerously incompetent, negligent, arrogant, careless, and undercredentialed physicians like Ajay Dhakal, I will continue to warn other women to avoid them. His next victim may not survive the typhlitic odds, in which case both he and UR Medicine will have blood on their hands.
Please don’t let it be yours.
































You must be logged in to post a comment.